
Hello March! Yes, March already! It's Myeloma Awareness Month. When I was first diagnosed, not many people I encountered knew what Multiple Myeloma was, (me included). But as my 8 years living as a myeloma patient have passed, I meet more and more people that have heard of myeloma, or know of someone diagnosed with myeloma. As I write this, I shake my head, forever having a difficult time connecting me to myeloma. It will always be an out of body experience for me. Still don't get how it found me...

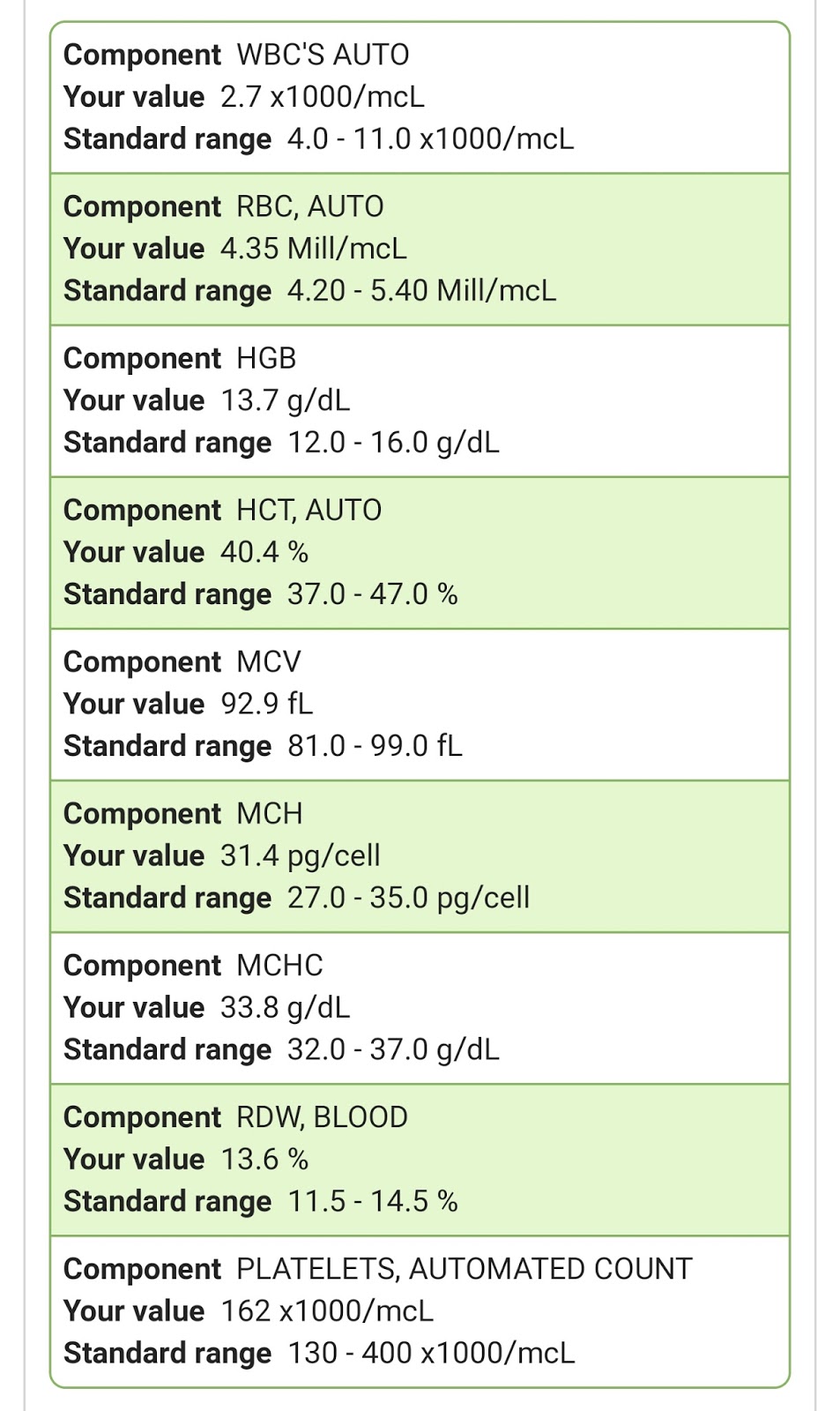
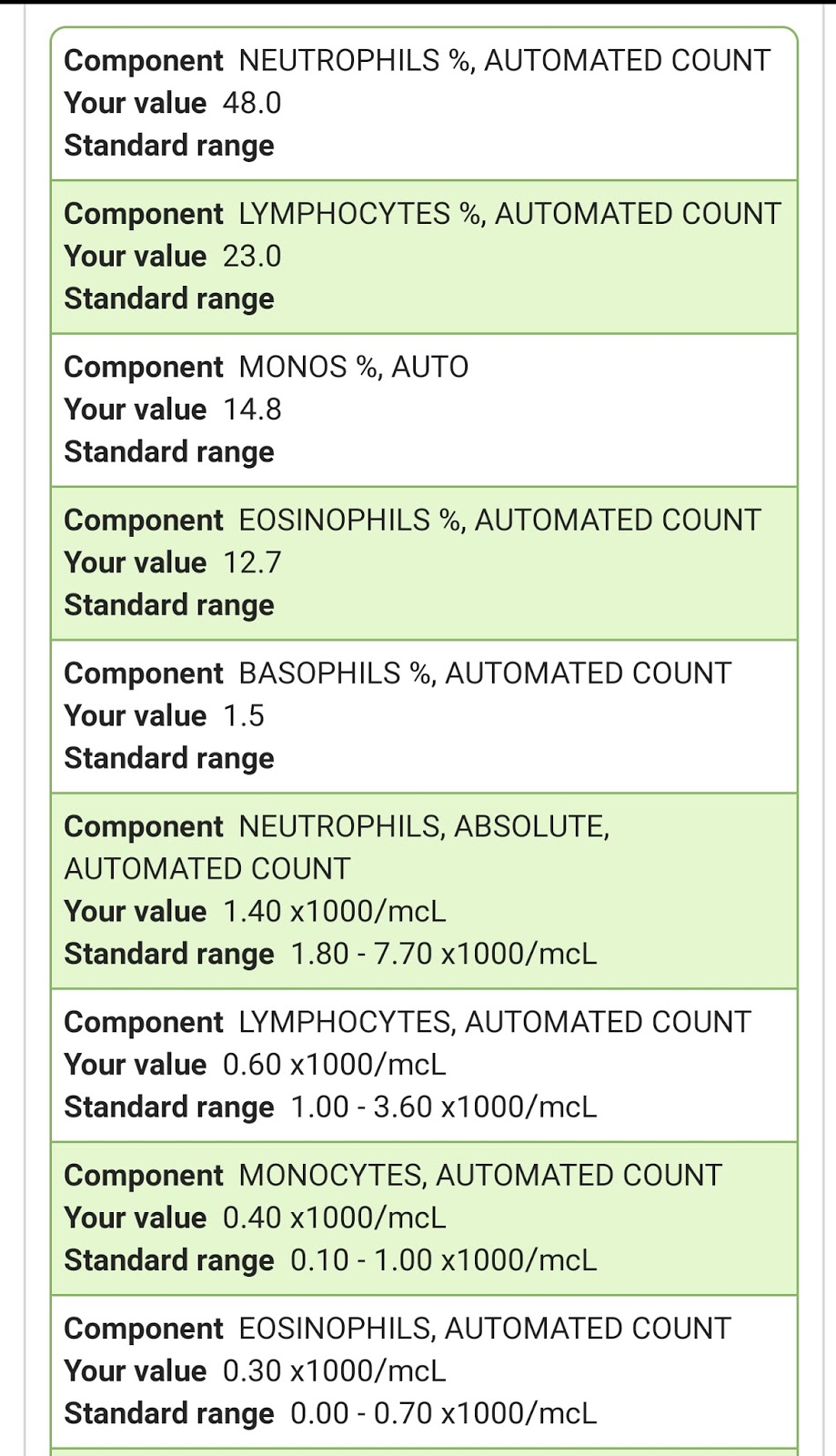
I did Labs yesterday, and will find out my myeloma stats on Monday March 12, when I have my next Dr appointment and Darzalex infusion. But I am able to see my CBC stats, organ function stats, and my Beta2 Microglobulin online. Here they are:
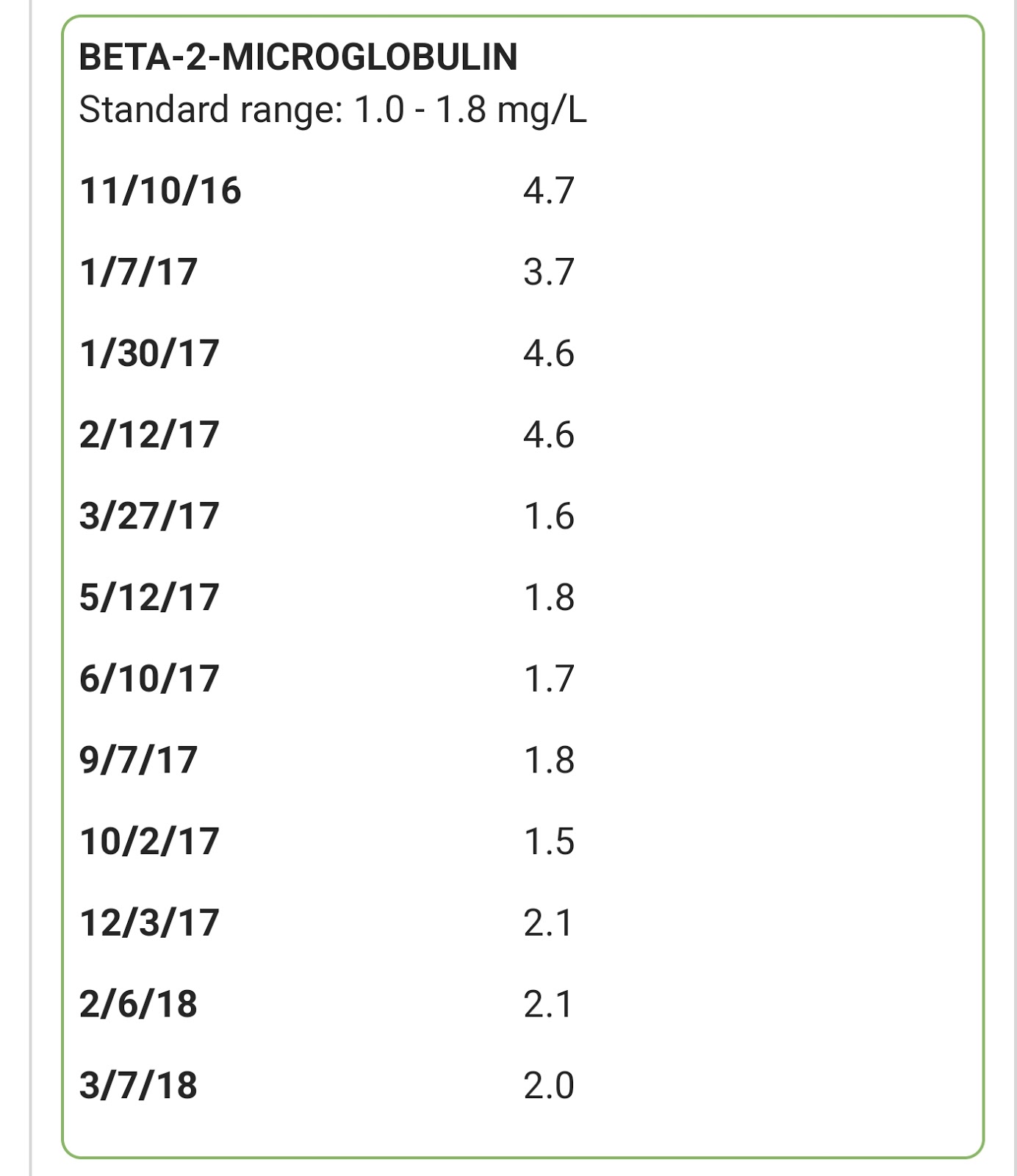
Not much, but I'll take any downward direction that comes my way :)
Crazy how high it was in 2009 at Dx @ 4.6, then in 2016, @ 4.7, then 4.6 just last year, prior to starting Darza, Pom, Dex! Still outside the "normal" range, but staying steady low-high for a year now, thank you triplet cocktail. Where did you come from myeloma, and how did you find me... Grateful for 8 years and counting, and for the "relative good health" I do have. Fatigue debilitates me. Headaches surprise me. Aches and pains annoy me. But thankfully I don't have the extreme GI issues I did with my previous treatments.
Life is busy with our new little rescue, who is more of a puppy than I expected. So adorable, so full of life, so healthy, so happy, so jumpy-bouncy, so much joy to share. He's doing great with potty training, as long as I make sure to let him outside regularly when he's inside. At night, I have him cozy in a soft tent-crate, and he seems to love that, and sleeps all night without a problem. When the weather's nice, all the doggies are outside for most of the day, so that makes it easy and natural for them.
I took little Jack to the Vet for his complimentary shelter rescue health exam. So funny how my life is so medical oriented on so many levels. He did great, and is in excellent health. Isn't he just so cute in his doggie seat-belt harness :)

Perfect little traveler and patient

Live happy, live well, and make a difference somewhere, somehow,
with someone or something as often as you can!
with someone or something as often as you can!
congrats on the new pup and congrats on the darzalex continuing to work.
ReplyDeleteHi Matt, thanks for checking in and commenting. I'm sure you saw I have your blog linked on mine :) Hoping you are doing ok, and I will check your recent post too. I think we're similar in timeline, and many treatments too. Yes, our new little rescue pup is hilarious and such a joy... and still a puppy-stage challenge lol. Thanks for commenting, and hope all is good with you!
Delete