
Hello end of June!
I have so many different directions I could take this post. My brain whirring like a summer fan. My thoughts are continual, non-stop, my questions persistent, my shock and awe still ever present. I just can't stop thinking about my situation and what has happened to me. Perhaps with many, the initial cancer diagnosis is the shock. Or initial chemo treatments rock one's world. Maybe losing one's hair, or extreme side effects from treatment, brings cancer's reality home. Maybe hospitalizations and stem cell transplants slam cancer's reality home. But for me, the longer I survive causes me to realize how serious and tentative my situation is. Yes I was blindsided by each event I mentioned above, but it's the LENGTH of time I've lived with myeloma, and the CONTINUOUS, unrelenting status of treating myeloma to STAY ALIVE, that never ceases to stun me and remind me daily, the insane circumstance I live with.
I am always processing how "out of control" I am of so many things in my life now. Prior to diagnosis, my body was basically my friend. Certainly not my enemy as it is now. I really didn't focus on my health much. Just took a lot for granted. Now, I can't help but focus on how little control I have over how my cells are continually cancerously morphing. How little control, actually no control I have, over deadly myeloma cancer cells multiplying defiantly, stealthly 24 7. I feel limited control over my future, my treatments, as cancer patients are completely dependent on medical science research for treatment pharmaceuticals, and on our medical professionals that determine what medications to treat us with. We like to think we are in control of our lives, and to degrees we are, but ultimately, not.
I can't help but remember my past days of carefree health, where I barely took any medication at all. I grew up with barely an aspirin in the house, as my parent's were "grin and bear it", anti medication type of people. Maybe we used aspirin for fevers, "Bactine" for cuts, but I don't recall knowing about Tylenol, Advil, cold/flu medications until I was a married adult. My parents took pride in having dental work done without Novocaine! I wasn't quick to give my kids pain meds either, and basically we were all really healthy people that didn't get sick or injured much, and didn't need pharmaceuticals. As I write this, I'm trying to recall what meds we did take. Allergy meds for all the seasonal polllens and irritants, and I developed hypothyroidism early in life, so I was on Levothyroxine for that. I can remember when people were over, someone might ask for a pain med, or allergy med, and I'd have to scramble to see if I had anything, and that it wasn't expired. We were so fortunate to be so healthy, carefree, and our bodies our friends.
 |
| Me, at about 14 or 15- So brave, no drama! |
How different my life is now, thank you myeloma.
A drawer in the kitchen holds all my myeloma meds, and supplementary pills. I have 2 pill boxes. The daily Monday through Sunday plastic boxes, that I once thought was only for "old people" or the "really sick". Guess I've joined that club. One box has Pomalyst, a half Benadryl, and a .81 aspirin, refilled 21 days. Then the other, Acyclovir, B12, D3. Also in this drawer is a variety of children's fast melt Tylenol and Advil, as well as adult strength. A variety of allergy meds, such as Benadryl, Claritin, etc. There are other Vitamins I irregularly take, a supply of Imodium left over from my "volcanic diarrhea" days, and older prescriptions for pain, muscle relaxants, nausea meds, antibiotics, etc. Most of those are expired, as I rarely need those. Our secondary "medicine cabinet" in the bathroom holds Salonpas, BenGay (for all my achy muscles), Pepto Bismal, Imodium, Tums, etc (that thank goodness I don't use those much anymore), and all of Jim's medications. And lest I forget, the refrigerator, holds several syringes of Zarxio (Neupogen), for when my WBC and ANC drops to Neutropenic status. But I know well, this is "Nothing" compared to my fellow myeloma warriors who have excruciating bone pain, continual infections, and worse side effects than I do...
But what I've really been processing recently, is my and all patient's lack of control over our treatment options, and ultimately the longevity of our lives. Yes we agree to myeloma treatments, but we are solely dependent on developed medications, what our Drs recommend and what insurance pays for. I know of so many myeloma patients that have run through all the "traditional" myeloma treatment options. Clinical trials are their only option, or the new Car T trials, or even sorting through past treatments, hoping to combine old and new meds for a new magic. See, choosing or agreeing to treatment is not like deciding what flavor of ice cream we want. We have to follow established research protocols, Dr analysis, pharma reommendations, insurance approval, etc. I understand "the why" for safety's sake,... but not being in control of my life, I will always struggle with.
Back when I was diagnosed, and prepping for my autologous stem cell transplant, I was in the "deer in the headlights" stage. I had immediately read till my eyes and brain hurt, but I really couldn't process what myeloma was, or what I would be going through. I felt informed, and fully trusted my medical team, so I eagerly did what they recommended. Yes, my perspective was always "less is more" and my Drs learned that I easily developed fairly serious reactions to meds at higher doses, so I never went beyond 10mg/15mg of Revlimid, etc. I didn't have much say regarding the stem cell process, but I survived that, and was very fortunate to have remission with maintenance Revlimid for 2 years. Without maintenance, myeloma came back in 2013 and I've been in constant treatment ever since.
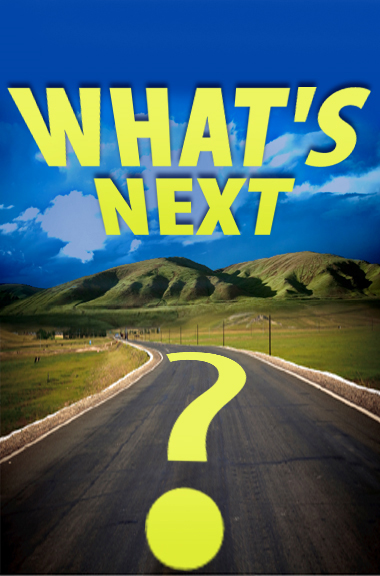
I've blown through uncountable rounds of Revlimid Dex (steroids), almost a year of Kyprolis Dex, and now Darzalex, Pomalyst, Dex, since March 2017. My IgA is climbing again, and both my local Dr and my SCT Dr are suggesting changes. First, increase Dex steroids from 20mg weekly to 40mg. IgA still climbed. Next, increase Pomalyst from 2mg/3mg alternating for the 21 day cycle, to 3mg only. From my recent labs for my my SCT appointment last week, my IgA climbed 300 points in 2 weeks. Ugh! So the conversation headed in the direction of what's next, what do I have left as treatment options and clinical trials...
Sorry, Nope, to clinical trials. Those scare me. With my luck, I'd wind up on a trial with the highest dose... and... well... yikes... nope... not there yet... Guess I'll brave up when I have absolutely NO options left. As I see it, I still haven't given Velcade injections a fair try, and then there's Ninlaro, the pill form of Velcade, and there's a variety of "approved" meds still on my menu, that I would brave up to try.
But before I change anything, I want to go back to the 2x monthly or weekly option of Darzalex. My IgA was almost "normal" when I was on the initial Darza Pom protocol. But for whatever medical, cellular, research reason, the protocol was determined to be: Weekly for 8 weeks. Then every other week, (2x per month), for another 8 weeks, then monthly until it fades and we become refractory to it. Well my perspective is, unless Darzalex has been determined to be toxic for extended periods, I just have to see for myself, if going back to 2x per month or weekly could still be my magic elixir. And this is where the "control" or "out of control" issue pushes my buttons... Shouldn't patients have a say so about this? If it worked before, heck, let's try it again. And I'll sign all the waivers necessary, since it's perhaps not a studied, approved protocol, which I can't believe the pharma developer isn't currently researching this option... maybe they are?
Myeloma stole my life, my body, my energy, my options, my choices... I just want want my voice to count...
Ok rant over... I wasn't going to write this much, but oh well... this is where my head's at right now. Very frustrated with myeloma owning me, medical science owning me, medical professionals owning my options, etc. So next week, at my Dr appointment and Darza infusion, this will be the conversation I will have, albeit edited, if my stats have continued to rise even more. Ugh, I hate you so myeloma for stealing my life, and making health, survival, medications, side effects, fatigue, pain, bodily functions, treatments, and being sick, the Focus of My Life!
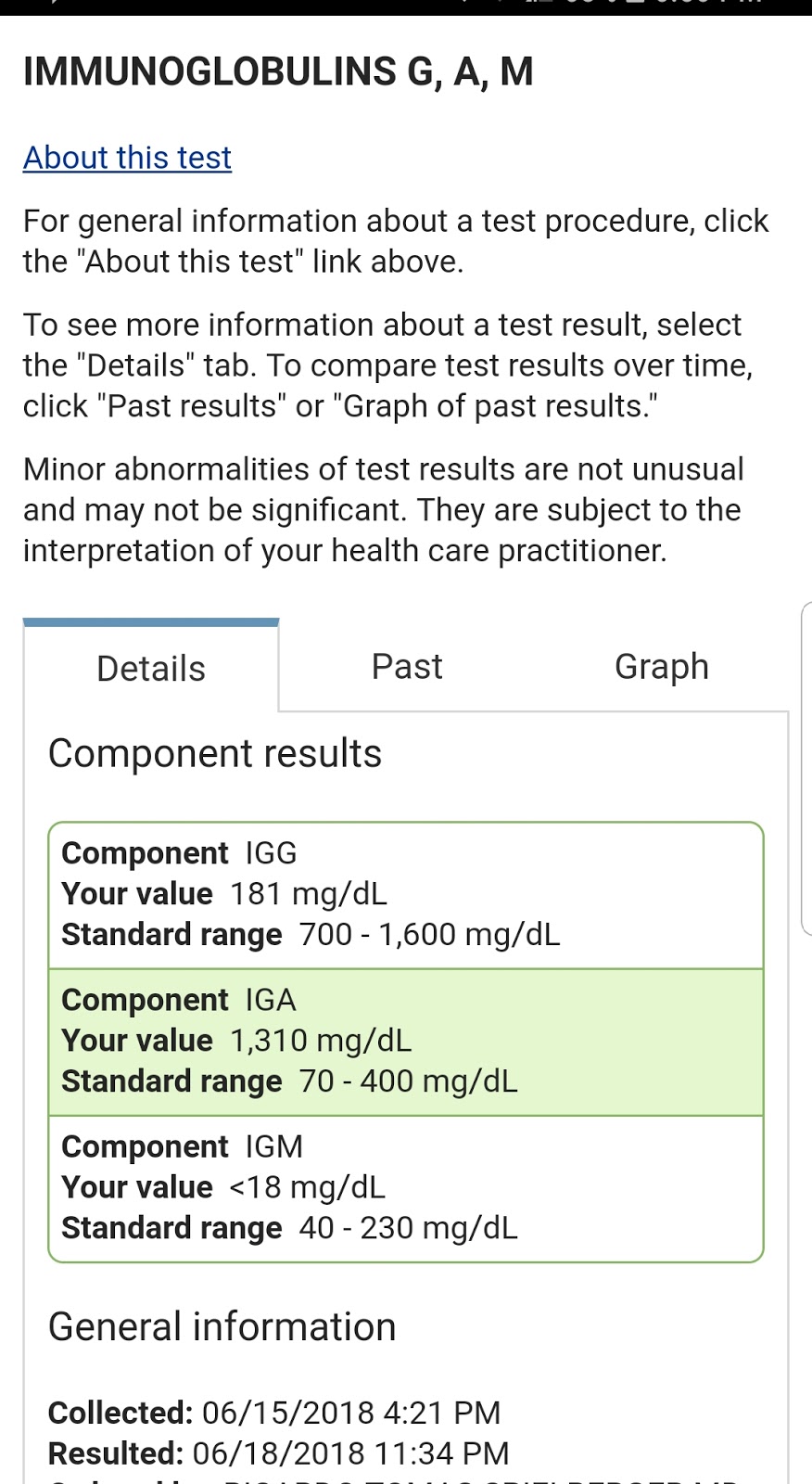
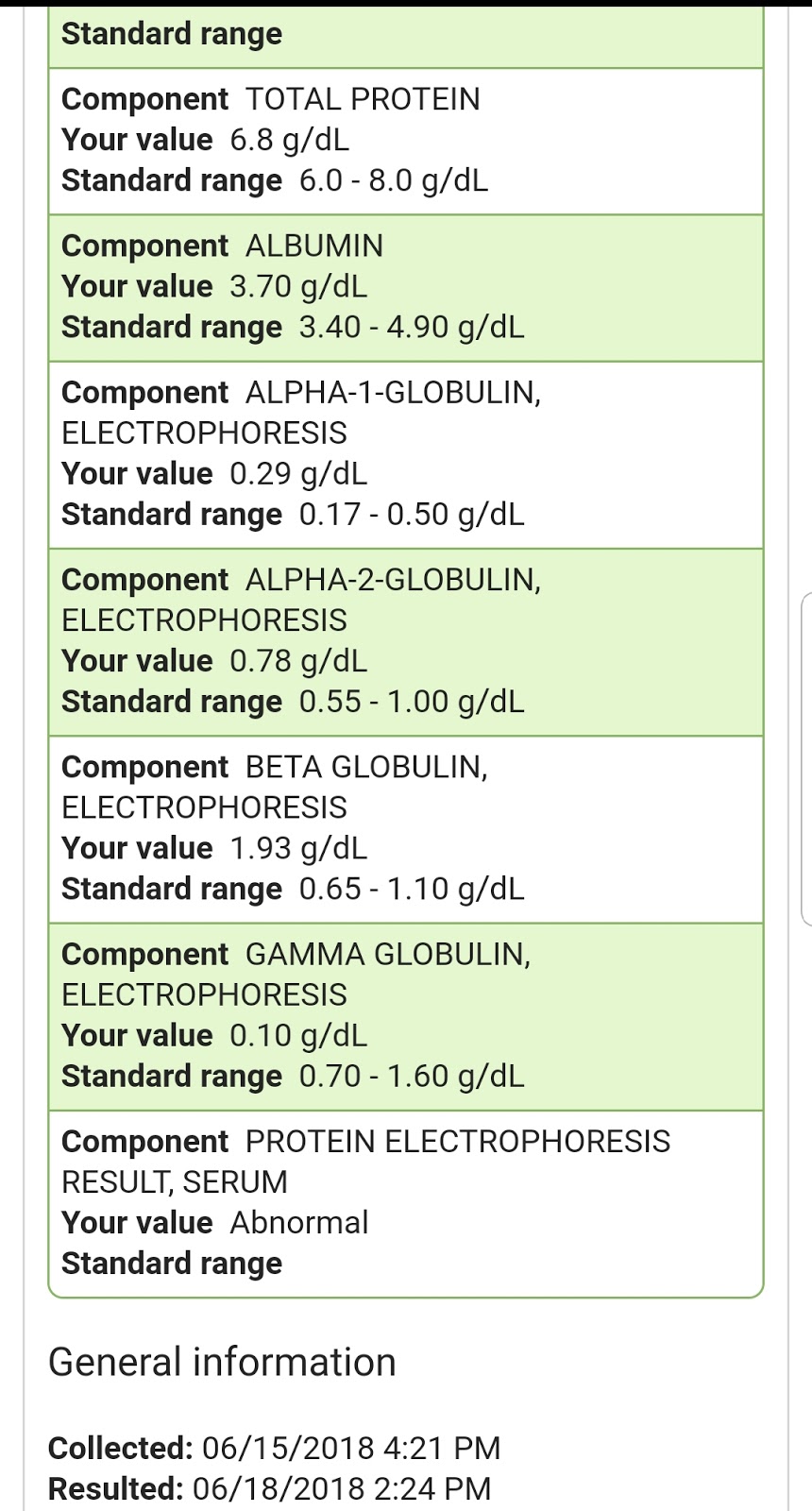
Here's my stats from last week, and I'll do labs again today for next Tuesday.
I apologize to all my fellow myeloma warriors out there who are having a much worse, and much more difficult time than me. I apologize for whining about my situation, knowing that so many of you are in a much more challenging situation than I am, regarding treatment options, insurance coverage, unsuccessful trials, etc. I apologize to anyone reading this who is in horrible pain, is out of treatment options, or who's circumstances make mine look like a vacation. I apologize to anyone who is on hospice or has a loved one in hospice. I used to think I was a pretty strong person, but myeloma has humbled me, and I'm not so strong and brave afterall. I don't do well in pain, or out of control of my circumstances, and I apologize for ranting like a whimp! May all of you find peace and happiness, and treatment success.


Live happy, live well, and make a difference somewhere, somehow,
with someone or something as often as you can!
I feel ya. I'm high risk and now my oncs are talking about next step: allo transplant. But that's absolutely terrifying (I've already had a tandem). The feeling of running out of options is breaking me psychologically as well, although I think we've already been broken in that regard from the get-go.
ReplyDeleteClinical trials sound tempting at this point.
Hi Conda, thank you for your comment! Yes, and not to add to your "fears", an Allo is not on my list. Congrats on your bravery for doing 2 SCTs! Wow, you are braver than me! And yes, we go from strong functional people to "broken" as you say. Amazing what a "continuing" aggressive, not in our control illness can do to us psychologically.
DeleteTell me more about your story, your Dx, treatments, and how long you've been battling. Wishing you the best of luck with all these crazy tough decisions and life adaptations :((
Thank you for reading my blog, commenting and letting me know your thoughts! Let me know what you decide!
Diagnosed Stage 3, high risk in 2015 May. I got a CR after the second transplant in March 2016 and immediately went on Rev maintenance until last year when it wasn't working anymore. Pomalyst and Dara started around spring/summer last year and it has kept my M-spike hovering around .1 , which is pretty good.
DeleteAlso was immediately put on Zometa because of severe compression fracture at T11, as well as one at T9. I couldn't take more Velcade because it caused severe neuropathy in my feet, which to this day, after 3 years, has caused basically non-functional toes, and an inability to walk barefoot without pain.
DeleteAnd finally, I was a bit of an athlete prior to this nightmare, a 10k runner, thrice a week casual jogger, and gym rat- who, during the year before diagnosis, occasionally did 50 pull-ups! Beast.
DeleteSo being essentially disabled has been traumatic and depressing and anxiety-producing.
Last thing! (friggin chemo-brain) Like you, I look absolutely normal, have gained 26 pounds (momma's cooking and too many smoothies), from 150 to 176. Sucks that pants don't fit. New wardrobed it all, though. I always tell my doc and nurse practitioner, "I'm FAT." To which they either say, " A little extra is good," or "No you're not! You look great!"
Delete