
Hello loyal readers and followers-

So I told my Dr I'd like to reduce the Pomalyst 3mg back to alternating 3mg with 2mg which I was doing since I began Darzalex, March 2017. I don't recall having this monstrous, indescribable pain prior to increasing Pom and enduring my CRAZY Zometa experience (see my July posts for those torrid details).So we'll see, as I begin Pom later this week, as thankfully I'm now on my 7 day Pomalyst break until Sunday. My Dr also ordered an MRI for me to follow up on my Pet CT Scan, to see what's going on with all my unbearable pain. Could this be the horrific bone pain most Myeloma patients mention? Or is this pinched nerves, muscle pain related to lytic lesion tumors, pinching or pressing on these areas? Or Sciatica? Ugh, who knows... but I do know, my tolerance and patience for side effects is waning after 9 years...
Yes, not a great idea to reduce dosage when my IGA continues to climb, but for me "quality of life" and less pain is more important to me than anything else.
I also asked my Dr about whether I should consider another SCT or Car-T, and she was surprised I asked, as in the past I was "No Way"... not suffering like that again... She did indicate that if was condsidering those options, now would be the time to do it, as my cancer levels aren't extreme, at this time... When I was originally Dx and prepped for my first SCT, my IGA was over 5700, M Protein was 4.3 and my first BMB showed 70% myeloma cancerous plasma cells. Hmmmm something to think about, but I want to see how my retro Darzalex plan works first. And I would probably want to experiment with all the myeloma treatments I haven't yet tried, or any of the new ones currently being approved... who knows... will cross that rickety bridge when I come to it...
So here's my life in statistics and pictures for you :))

I'm up about a 100 points from last month
Not happy about it, but not panicked about it either
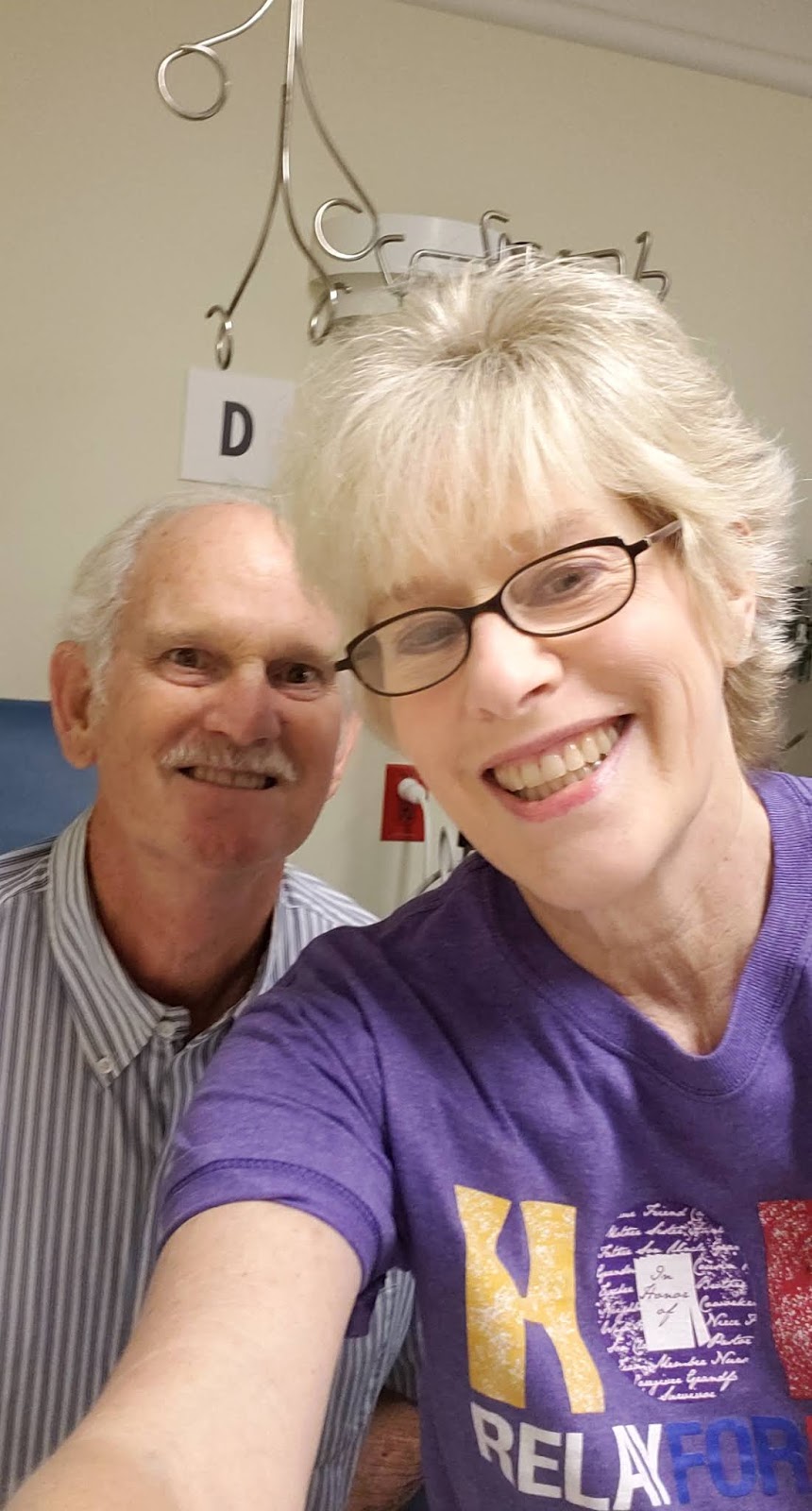
Myeloma pal and neighbor Gary
He was Dx about 8 months after me
and we've been thru very similar treatments,
altho he's IGG and Kappa Light Chain MM
He's currently preparing for a Car-T trial with City of Hope

Best Volunteer Ever, Karen
She takes great care of me and all the patients
and we have some great laughs about life
and when my Benadryl infusion meets my 40mg Dex steroids!
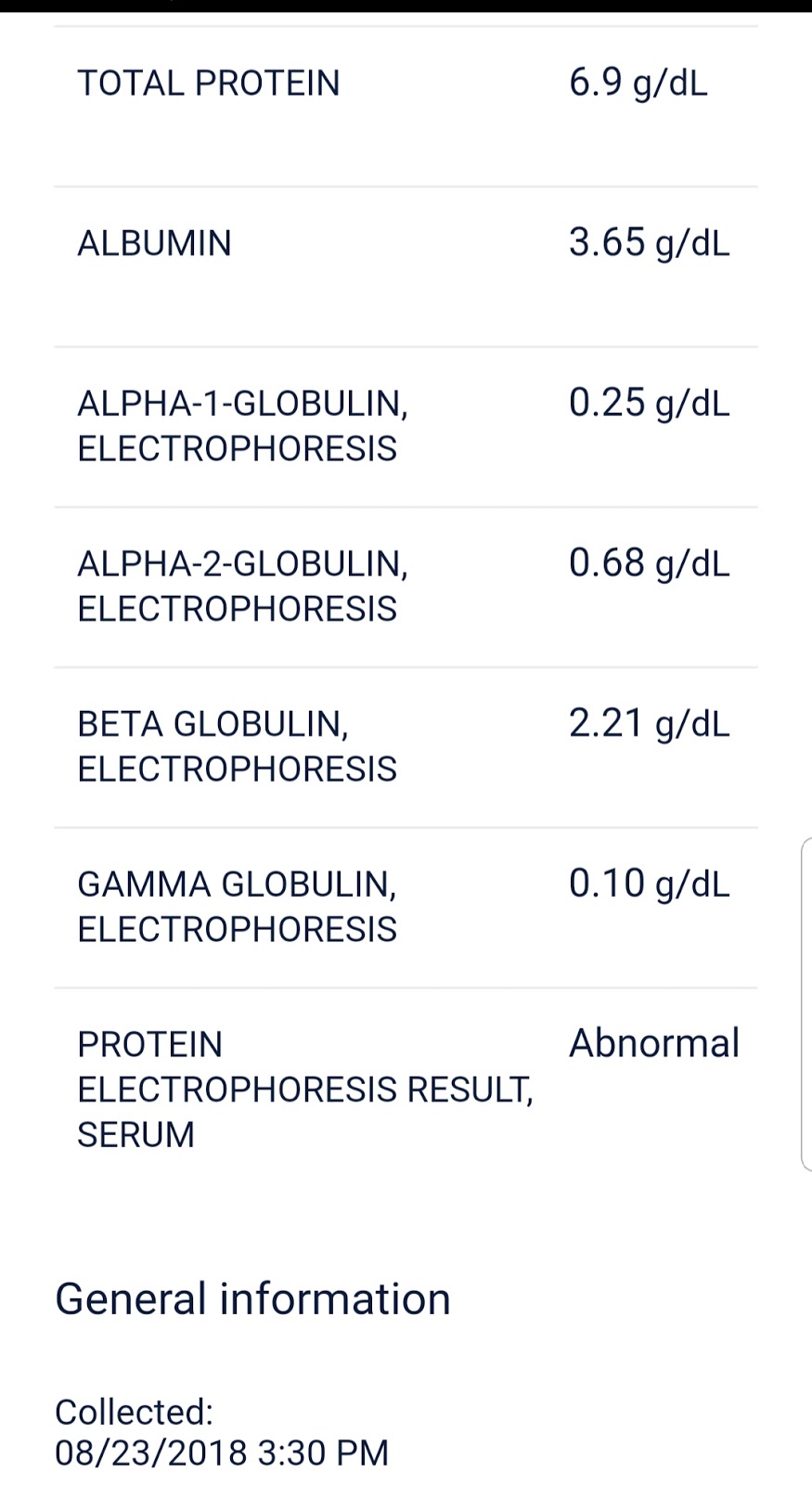
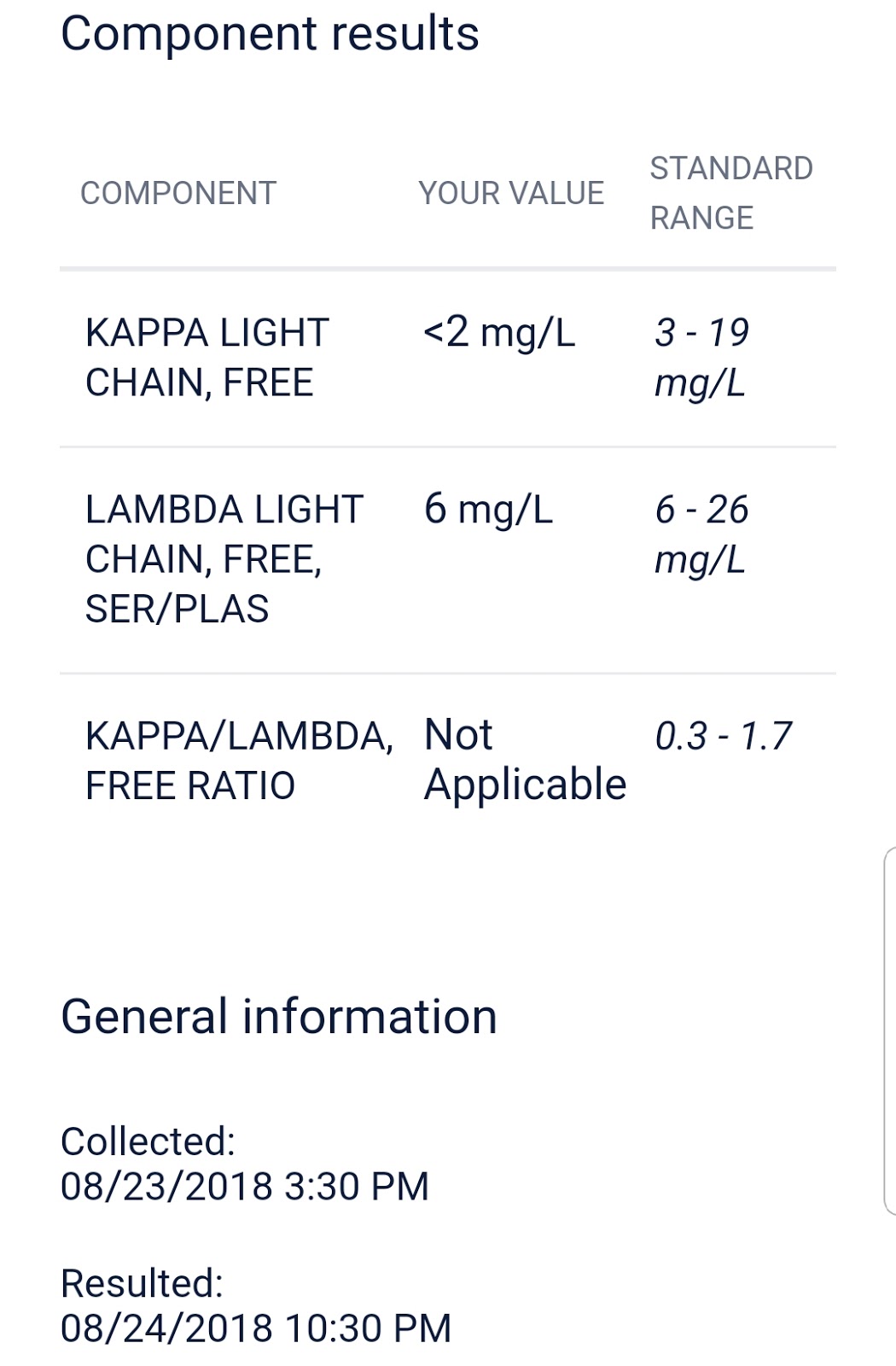
Still no visable M Protein
so perhaps Darzalex properties suppress it?
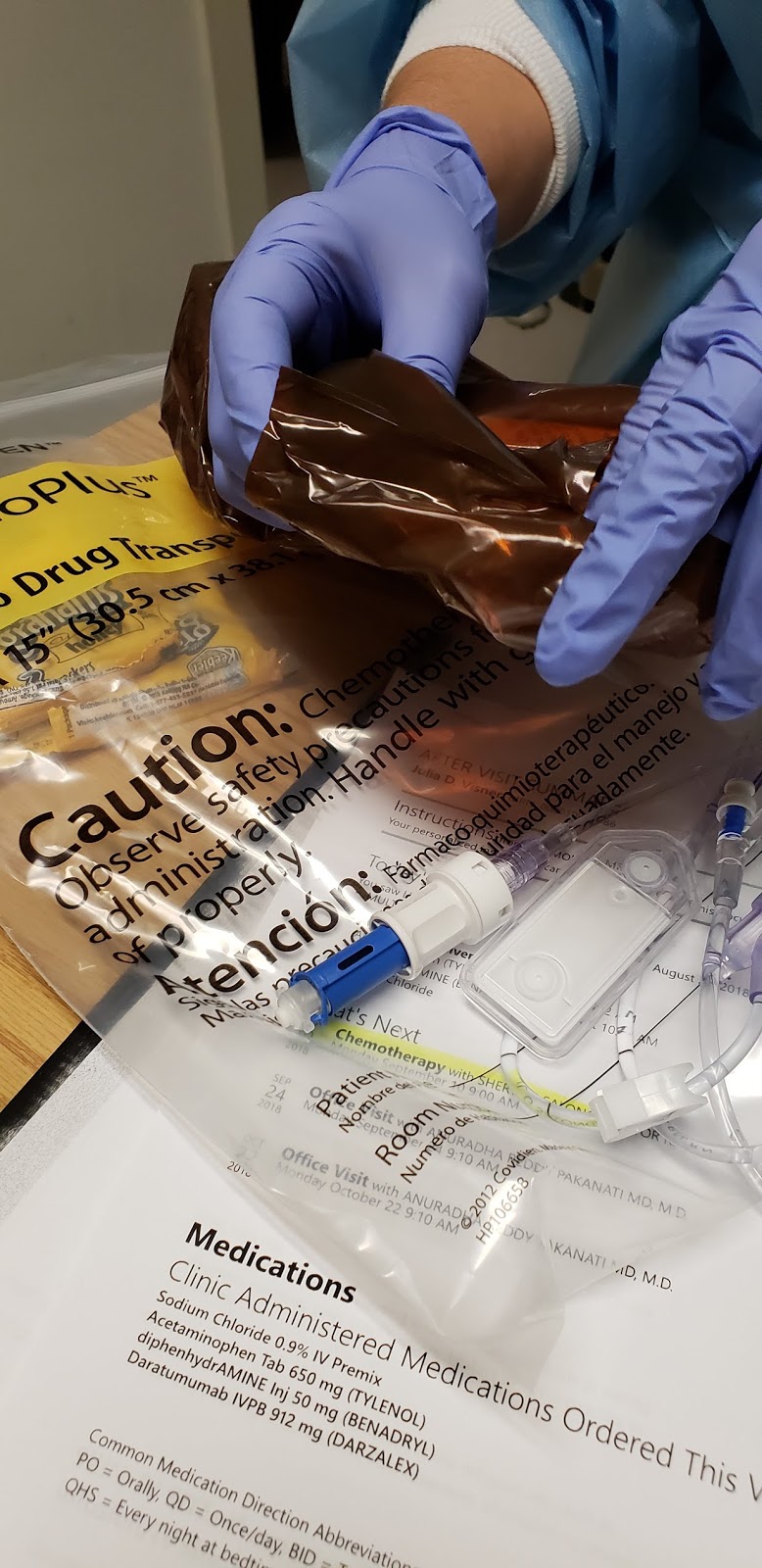
Here comes Darzalex
My awesome Nurse Josie
who always laughs at my Selfie taking
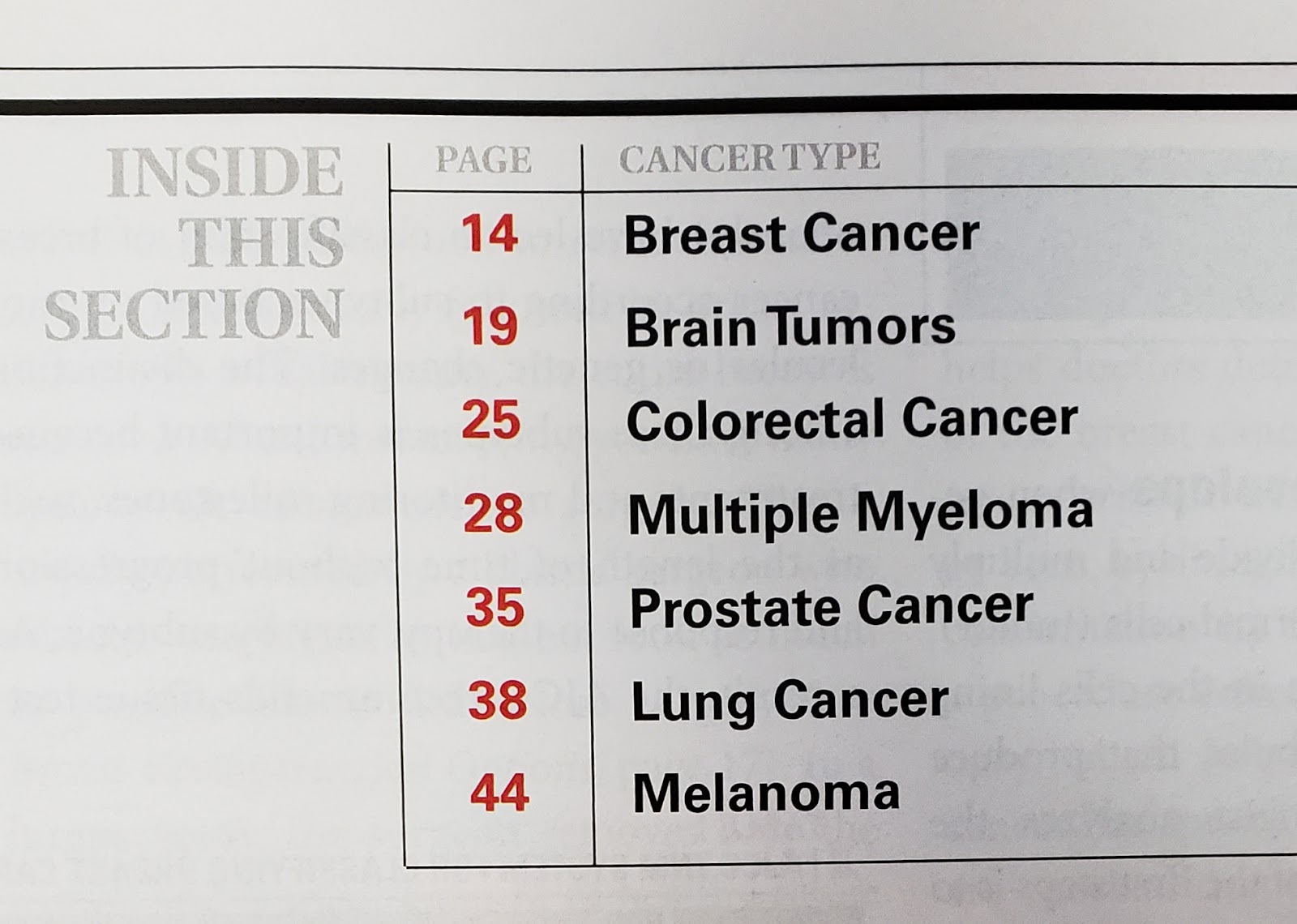
I picked up a Cancer magazine while waiting today
and was stunned to see Myeloma featured
with all the "popular", more common cancers
Sadly tons of people are being Dx everyday with Myeloma
It's no longer a "rare" unknown cancer....
And that's my story for the last post of August, 2018. I'm already referring to my journey as "almost 9 years now", when I meet people and share my story. I think it's pretty dang amazing that I'm still here, and as "functional" as I am, 9 years later. It's probably longer than 9 years, as when looking back on all my early symptoms I denied in 2008, 2009, I've probably had Myeloma, or Smoldering Myeloma for a much longer time...
I attended the IMF seminar this past weekend, which is very informative and well organized, has great Myeloma Specialist speakers, and I met some great fellow MM-ers. My almost 92 year old dad had a pacemaker installed this past week. I did circles around the barn last night past darkness, as I felt so bloated and stiff from sitting all day for my loooong Darzalex infusion, then sitting driving home, then sitting at dinner with myeloma buddy Gary and his wife. We took advantage of our energy blast and appetite rage from the lovely Dex steroids! I've gained a few pounds recently from eating ice cream on hot summer nights and other sweet goodies, so time to rein in my "F cancer" attitude and go back to obsessive calorie counting LOL. Wish I had the energy to walk more often, but my loooow WBC and ANC and extreme Fatigue most often prevents me from doing much physically. Ugh, to think what I used to do... Oh, I walked into several black widow webs, and killed a BIG one last night... I always feel bad snuffing out a life... but it's me or them, and I choose me, and not being bit!
Hoping all is good with all of you and yours, and you've had a nice summer. I love when you comment and let me know you're out there, and of course I love hearing your life story too. Thank you to all of you that loyally follow my posts regularly, and thank you to those that have just recently happened upon my story.

No comments:
Post a Comment